France
France Australia
Australia
What is a shoulder dislocation?
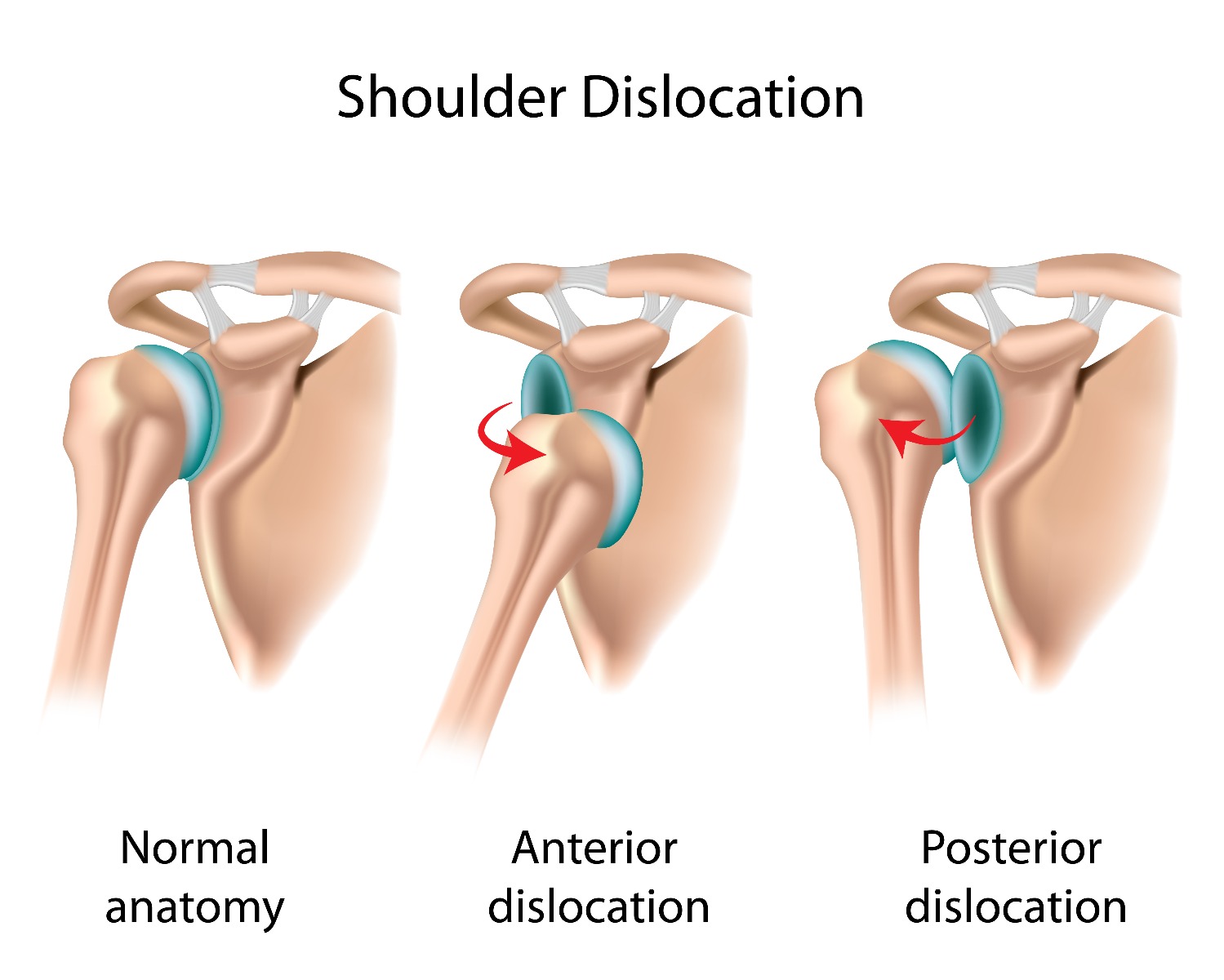
There are two types of shoulder dislocations. A partial dislocation (sublaxation) occurs when the head of the humerus (arm bone) is partially out of the scapula (shoulder bone). A complete dislocation means the head of the humerus is all of the way out of the scapula. The shoulder dislocation can be anterior (forward, 98% of displacements), posterior (backward, 2% of displacements), or inferior (downward, rare).
The Golf Ball Analogy

You can picture your shoulder joint as a golf ball sitting on a tee. The ball would be the head of your humerus (arm bone) and the tee would be the glenoid fossa of your scapula (shoulder joint socket). The ball is larger than the tee making it unstable. Similarly, your shoulder joint allows a lot of mobility and range of motion, but this sacrifices stability because the head of the humerus is large. Your surrounding shoulder muscles (rotator cuff, biceps, deltoids) help hold the joint during movement, help the ball stay on the tee, but this system doesn’t work as well when your muscles are fatigued.
Causes of Dislocation
The most common cause of a first time shoulder dislocation is a traumatic injury, such as a forceful collision, sudden wrenching movement, or fall on your outstretched arm. These account for approximately 95% of shoulder dislocations while the other 5% are atraumatic. This means they are caused by minor incidents like raising your arm or putting it in a certain position while sleeping. People with atraumatic dislocations have abnormalities in their muscles and connective tissue around the shoulder.
Symptoms
- Visible deformation (shoulder looks “out-of-place”)
- Intense shoulder pain
- Swelling and/or bruising
- Inability to move the joint
- May cause numbness, tingling, or weakness in your arm or neck
- Shoulder muscles may spasm due to pain
See a medical professional right away and don’t try to put your shoulder back in place yourself.
Recurrence Rates
7 out of 10 people will dislocate their shoulder again within two years of the first dislocation. Recurrence is much more common in adolescents, though first time dislocation rates are similar for all ages.
Shoulder re-dislocation occurs in:
- 66-100% of people 20 years old or younger
- 13-63% of people 20-40 years old
- 0-16% of people 40 years old or older
Dislocations in Athletes
Shoulder dislocations are common in athletes. Overhead sports players and those who experience forceful crashes are particularly at risk.
This includes sports like:
- Rugby
- Hockey
- Football
- Cycling
- Volleyball
- Tennis
A shoulder dislocation can occur with much less trauma if it is a recurrent injury or if your shoulder muscles are weak.
Pain Relief
After a doctor reduces your shoulder (pops it back into place) your severe pain will be relieved, but you will still have some aches and pains. You can recieve fast relief using a topical analgesic, like Biofreeze, on the area. Hot and cold therapy can also help with pain relief. Talk to your doctor about whether heat or cold is better for your dislocation and use what feels best. Heat can be helpful to loosen your shoulder prior to physical therapy while cold can help relieve any discomfort after exercise. A shoulder wrap can offer both forms of therapy and allow you to ice your shoulder post-reduction.
Shoulder Immobilization
Your physician will probably recommend a sling after your shoulder reduction. This helps keep your shoulder immobilized in the best position while it heals. A sling is commonly worn for 1-3 weeks. Follow your doctor’s instructions on how long you should wear yours.
You might need a shoulder brace during recovery. The brace supports your shoulder while it heals and offers light compression to help reduce inflammation. Most braces still allow shoulder movement so they can be worn during strengthening exercises. You can wear a shoulder brace after your recovery to help prevent dislocations in the future. It offers support and prevents your shoulder from moving into the vulnerable range. A brace is more likely to be recommended if this is a recurring injury.
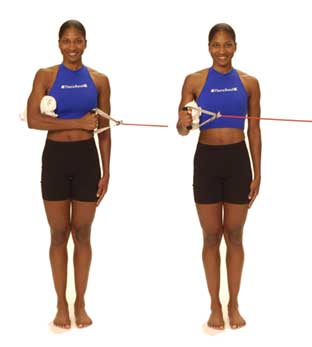
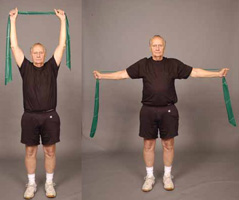
Rehabilitation Exercises
Physical exercises can help prevent long-term shoulder instability problems. Using an elastic resistance band or tubing is an affordable, flexible way to stretch and strengthen your shoulder. You should also use your TheraBand resistance tubing to build up surrounding muscles and help avoid another dislocation.
| Shoulder Rotation at 0° Exercises | |
|
TheraBand Internal Rotation
|
TheraBand External Rotation
|
|
|

| Shoulder Rotation at 90° Exercises | |
|
Internal Shoulder Rotation
|
External Shoulder Rotation
|
|
|


| Exercising Surrounding Muscles | ||
Bicep Curls  |
Lat Pull Down |
Chest Press  |
|
|
|
Surgery
Surgical intervention or arthroscopic shoulder treatment is only recommended by doctors if conservative treatment (sling, brace, physical therapy, etc.) fails. It may also be necessary if the surrounding tendons, ligaments, bone, muscles, or nerves were injured at the time of the dislocation or if your shoulder is dislocated repetitively.
References
Gaballah, A., Zeyada, M., Elgeidi, A., & Bressel, E. (2017). Six-week physical rehabilitation protocol for anterior shoulder dislocation in athletes. Journal of Exercise Rehabilitation, 13(3), 353–358. Retrieved from http://bit.ly/2ptywFZ
Hayes, K., Callanan, M., Walton, J., Paxinos, A., & Murrell, G. A. C. (2002). Shoulder Instability: Management and Rehabilitation. JOSPT, 32(10), 497–509.
Medical Disclaimer: The information provided on this site, including text, graphics, images and other material, are for informational purposes only and are not intended to substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or other healthcare professional with any questions or concerns you may have regarding your condition.